White Paper
The Pelvic Floor Muscle Trainer You Need
Diane K. Newman, DNP ANP-BC, FAAN
|
Sandra is a 53-years-old peri-menopausal, middle school teacher with three grown children. To stay in shape and to relieve stress, she plays on a women’s tennis team, a lifelong exercise. All her children were vaginal births and she had “tears” with each, some worse than others. At an annual well-care appointment, her health care provider noticed that she was wearing a pad attached to her underwear. When her provider inquired about the need for a pad, Sandra became very embarrassed. She reluctantly reported “a little” urine loss when playing tennis and a pad helped. Sandra felt that she was managing the leakage with little problem, but asked her provider, “Will it get worse?” Sandra’s health care provider said that urine leakage, called urinary incontinence, can get worse after menopause. But Sandra can stop that progression by following a training program to strengthen her pelvic floor muscles. Pelvic floor muscle exercises, or Kegel exercises, have been shown to be effective in preventing and decreasing incontinence. However, many women have a difficult time finding the right muscle to strengthen and end-up exercising the wrong muscle. To be effective, isolating and training the correct muscle is important. Are there ways to help Sandra be successful in performing effective in-home pelvic floor “Kegel” exercises? |
Introduction
Urinary Incontinence: A byproduct of weak pelvic floor muscles
|
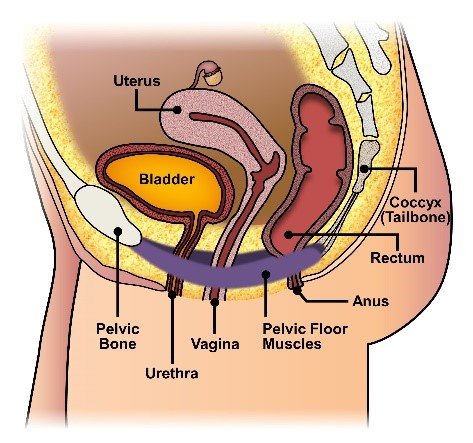
Figure 1: Pelvic Floor Muscles |
Sandra is not alone. Of the 25 million adult Americans suffering from some form of urinary incontinence, over 70% of those are women.[1] One in four women aged 18 years and older, experience loss of bladder control, resulting in accidental loss of urine.[2]
|
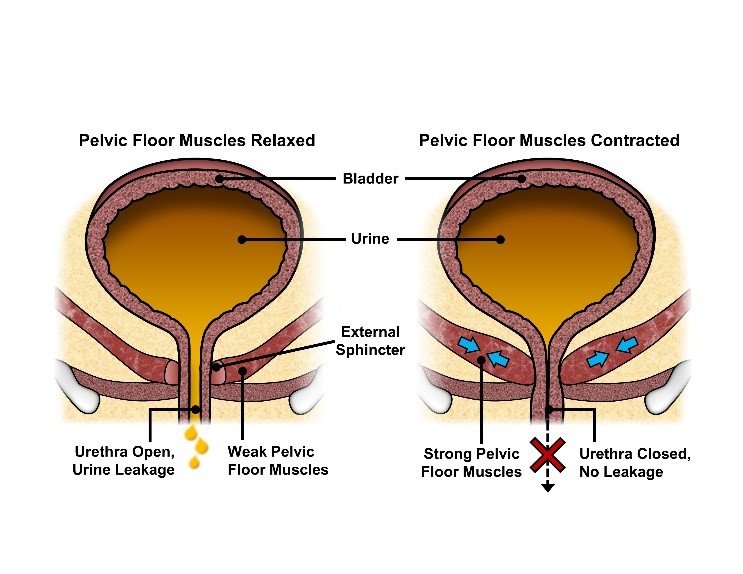
Figure 2: Strong pelvic floor muscles (left) and weak pelvic floor muscles (right) |
Like Sandra, approximately half of the women who suffer from urinary incontinence have stress urinary incontinence (stress UI), which is the leakage of urine with effort and physical exertion. Urine leakage can occur with a cough or laugh, with activity such as picking up a child, or during any type of exercise (e.g., running, playing tennis). Urinary incontinence in women is a real barrier to regular physical and fitness activities, can lead to diminished social contacts, and adversely affects quality of life.[3]
The pelvic floor is a group of muscles and ligaments that
form a hammock to support the pelvic organs – bladder, uterus, and bowel – as well as provide core stability and postural support. (Figure 1) These are the muscles that surround the vagina and support the voluntary urinary sphincter, which is a valve that prevents urine from leaking.
Pregnancy, menopause, surgery, and aging can weaken the vagina and surrounding pelvic muscles. The bladder can drop (prolapse), therefore changing position, which prevents the urethra from closing properly (Figure 2). With a weak vagina and pelvic floor muscles, women may experience prolapse of pelvic organs, urinary and bowel incontinence, sexual issues (e.g., painful intercourse, lack of sensation), and back and pelvic pain. [4]
Although increasing age is the most widely accepted risk factor for pelvic floor muscle weakness; pregnancy, and childbirth (particularly vaginal births), genetics, obesity, previous hysterectomy or pelvic surgery, chronic coughing from pulmonary disease or smoking, diabetes mellitus, frequent heavy lifting, and menopausal status are known to increase susceptibility.[5] [6]
Urine leakage is not a normal part of aging and treatments are available to reduce or eliminate the problem. These treatments include lifestyle changes (e.g., fluid and dietary modifications), toileting programs (e.g., bladder training, double voiding, scheduled toilet trips), and stress or urge “tricks” (e.g., contracting the pelvic floor muscles to prevent urine leakage or to lessen bladder urgency). There are more complex therapies (e.g., Botox, acupuncture, nerve stimulators, surgery), but many women are not interested in these as they carry more risk. Medications are available only for urgency UI and overactive bladder symptoms of urgency and frequency.[7] Treatments focused on strengthening the pelvic floor muscles play an important role in the healthy management of pelvic conditions.4 Multiple studies suggest a correlation between toned strong pelvic floor muscles and enhanced sexual health and sensitivities.
What are these exercises? In the 1950s, Arnold Kegel, an obstetrician and gynecologist in Southern California, developed exercises consisting of repeatedly contracting and relaxing perineal-area muscles to strengthen the vagina and pelvic floor.
Dr. Kegel used a biofeedback device, called a perineometer, an intravaginal pressure probe. These pelvic floor muscle exercises, initially referred to as “Kegels,” work to improve the function of weak and atrophic muscles that support the vagina, urethra, and bladder. Kegels are an essential element of pelvic floor muscle rehabilitation and performing them at home poses no drawback to any other therapies. Clinical recommendations from several professional organizations underline the importance of consistent pelvic floor muscle training for managing urinary incontinence (Table 1), bladder urgency and frequency.
Table 1: Clinical Recommendations for Use of Pelvic Floor Muscle Training
| Association | Clinical Recommendation |
| International Urogynecological Association/ International Continence Society | Joint report presents pelvic floor muscle training as conservative, non-pharmacological management of female pelvic floor dysfunction.[8] |
| Canadian Urological Association | Pelvic floor muscle training should be incorporated into the activities of daily life to promote compliance and adherence. Continuous training is needed to maintain the gained strength of the pelvic floor muscles.[9] |
| Society of Obstetricians and Gynecologists of Canada | Recommends use of pelvic floor muscle training for stress UI.[10] |
| American College of Obstetricians and Gynecologists | Pelvic floor muscle exercises may be done 6-weeks post-partum.[11] |
|
American College of Physicians
|
Pelvic floor muscle training is recommended as the first-line of treatment in women with stress UI.[12] |
| International Consultation on Incontinence |
Pelvic floor muscle training should be offered as first-line conservative therapy to women with persistent UI symptoms three months after delivery. (Grade of Recommendation: A) Supervised pelvic floor muscle training should be offered as a first-line conservative therapy for women of all ages with urinary incontinence (Grade of Recommendation: A) An ‘intensive’ pelvic floor muscle training program (in terms of supervision and exercise content) is likely to increase the treatment effect. (Grade of Recommendation: B) [13] |
Challenge
|
After receiving pelvic floor muscle exercise instructions, Sandra attempts to do the exercises at home. Without accurate feedback, Sandra is not certain she is doing them correctly and is worried she is not contracting the correct muscle. Seeing no immediate results, she becomes discouraged and eventually stops doing them altogether. At a follow-up visit with her provider, Sandra expresses frustration about the lack of results. She thinks her muscle is too weak, because she cannot feel it when she tries to do a muscle contraction. She reports increasing inconvenience and embarrassment caused by the urine leakage. Sandra is voicing a common complaint—the inability to isolate the muscle. How can Sandra be certain that she is strengthening the right muscle correctly? |
When Kegels are performed correctly and regularly, studies show women, across all age groups, experience up to 70% improvement in the symptom of stress UI.[14] In fact, one study shows women who performed pelvic floor muscle exercises were five times more satisfied with their bladder status.[15] However, women report the lack of confidence in performing the exercise correctly, the time commitment needed, and inadequate instruction as factors in adhering to a pelvic training program.[16]
For many health care providers, this rings true. Nearly a quarter of health care professionals surveyed believed a significant barrier to women implementing positive health changes was that women were unsure what to do to be healthier.[17] The challenge is instructing and motivating women with stress UI to perform in-home pelvic floor muscle exercises correctly and consistently.
Requirements of a successful pelvic floor muscle training program
A successful pelvic floor training program parallels any effective exercise regimen. It requires proper muscle movement – muscle isolation and feedback – with consistent repetition and increased resistance.4
First, women need to be able to recognize the pelvic floor muscle to sense the effort needed to move and contract the muscle. Studies show that up to 30% of women exercise the wrong muscle group due to poor muscle identification and isolation.[18] Providing cues or feedback (e.g., audio, visual, vibration) as the woman contracts the correct muscle, facilitates the ability to isolate the pelvic floor muscle and sense muscle contraction. She then learns to control the pelvic floor muscle by responding to visual or auditory signals generated through the activity of an internal physiological process.[19]
Next, women need to “work out” the pelvic floor muscle as they would any muscle with strength training (e.g., weights, resistance) to increase muscular strength, tone, and endurance. Expert clinicians recommend increasing pelvic floor muscle exercise intensity (e.g., resistance, duration, sets) to gain earlier and further benefit. Dr. Kegel explained that progressive resistant exercises are the most effective physical therapy to correct muscle disuse and atrophy and restore normal function.18
Lastly, women need to perform these exercises regularly. Evidence is overwhelming that regular pelvic floor muscle exercises positively affect pelvic health and can improve – and even prevent – urinary incontinence and associated bladder symptoms. Experts vary on the recommended frequency of these exercises for reported improvement in symptoms. Dr. Kegel recommended pelvic floor muscle exercises be performed multiple times each day, for several minutes at a time, for one to three months. Today’s experts recommend a more intensive exercise program for at least six months.[20] [21]
The compliance factor
A critical factor in the outcome of a successful pelvic floor muscle training program is the patient’s willingness to perform the exercises correctly and consistently. Theories of motivation emphasize the positive role that perceived competence in a physical activity can intrinsically motivate a person to continue that activity. Research shows that mastering a goal is most strongly related to positive outcomes, such as increased self-perception, autonomous motivation, enjoyment, and behavioral persistence.[22] A successful strategy, used by health care professionals to educate women on their proficiency with pelvic exercises, is the use of biofeedback as part of a training device. 19 Delgado et al.,16 noted that the use of a pelvic floor muscle training device appeared to help women gain confidence that they were doing the exercises properly plus motivated them to continue.
Recent technological advancements have resulted in the availability of numerous home-based, biofeedback-assisted pelvic training devices. These devices are purported to aid women in performing Kegel exercises properly. However, many of these devices fall short in offering progressive resistance and accurate feedback with standardized instruction. The need exists for a practical and safe pelvic training device with these features to better instruct and motivate women with urinary incontinence and associated bladder symptoms in performing in-home Kegel exercises correctly and consistently.
Solution
| In a follow-up call, Sandra reports having given up on pelvic floor muscle training and has stopped playing tennis due to increased stress UI leakage. She is encouraged to perform the pelvic exercises using a pelvic training device. She is asked for a one-month commitment to try the device and measure results. What could help Sandra see results so she will be persuaded to continue pelvic floor muscle training and possibly remove barriers to a healthier lifestyle? |
|
Figure 3: Vibrance™ Pelvic Trainer without sleeve 2012 Medical Design and Excellence Award for design and effectiveness (Silver Winner for design and engineering in the Over-the-Counter and Self-Care Category) |

The Vibrance™ Pelvic Trainer from Bioinfinity USA is a FDA-cleared intravaginal medical device, available without a prescription, for strengthening pelvic floor muscles to improve pelvic health and quality of life. This clinically proven, easy-to-use pelvic training device enables women to properly perform Kegel exercises at home so as improvement in muscle strength, tone, and bulk is achieved.
Easy-to-use: Shaped and inserted like a tampon, the Vibrance Pelvic Trainer is a force-feedback device. It consists of a main cylindrical biofeedback probe made of body-safe, medical-grade silicone rubber (Figure 3). The probe senses body-force and transmits gentle vibrations when muscles are correctly engaged (contracted). The Vibrance Pelvic Trainer’s simple, safety-tested design requires minimal set-up and allows for easy cleaning.
|
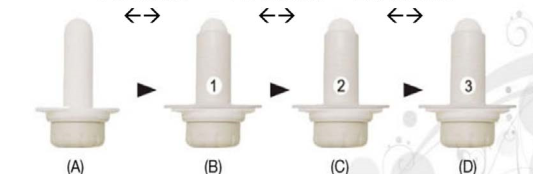
From A to D: (A) Higher sensitivity requires lower force to activate Figure 4: Progressive Resistance Training Sleeves |
Accurate performance biofeedback feature: The Vibrance Pelvic Trainer uses a patented biofeedback technology to help women know, with certainty, they are exercising the right muscle correctly. When the vaginal muscle squeezes around the force-sensitive probe, triggering a vibrating sensation in the vagina and to the pelvic floor muscles. This vibration engages only when the device is in contact with the correct muscles.
Progressive physical resistance feature: The Vibrance Pelvic Trainer offers women the ability to strengthen pelvic floor muscles beyond normal contractibility strength with an outer sleeve in three degrees of resistance for different training intensities (Figure 4). Each Training Sleeve is biocompatible and hypoallergenic. Although the main probe itself provides a certain level of physical resistance, when one of the three Training Sleeves is placed over the probe, the pelvic floor muscle needs to squeeze harder against the stiffer barrier of the sleeve to generate the sensation in the vagina. The woman starts with the main unit, which is designed to help her adjust to isolating and activating the correct muscle group. This physical resistance and increased intensity enable the women to progressively condition and build muscle strength, tone, and endurance.
Audible-guided training feature: In addition to providing a vibrating feedback, the Vibrance Pelvic Trainer includes an audio feature that guides the women through the optimal duration and repetition of contracting and relaxing the pelvic floor muscles using distinctive signals, or “beeps,” to achieve the best results when exercising the correct way. This routine consists of long and short intervals to engage both the fast twitch and slow twitch muscle fibers. Additionally, it reinforces when to pause, allowing the muscle to rest, which is essential for muscle endurance.
Results
| Sandra has used the Vibrance Pelvic Trainer for one month. She reports that the audible-guided training and biofeedback features have helped her learn to engage the correct muscles. She is now using resistive training sleeve #2 and feels it is helping her pelvic muscles increase in strength. She reports improvement and appears motivated by early results to continue training and progress to the next level of strength and endurance. Measuring and seeing results has encouraged her to continue to train her pelvic floor muscles. |
Vibrance Pelvic Trainer Efficacy Research
To compare the effectiveness of doing pelvic floor muscle exercises with and without the Vibrance Pelvic Trainer, 40 women (age 18 or over) suffering from stress UI were selected as part of a pilot prospective, randomized trial.[23] Patients were randomized with 19 assigned to a control group (pelvic floor muscle exercises alone) and 21 assigned to the Vibrance Pelvic Trainer group (exercises with the Vibrance Pelvic Trainer). Both groups underwent 16 weeks of training, with self-assessments and strength testing at weeks 0, 4, and 16. All women in the Vibrance Pelvic Trainer group stayed in the study. The control group had three women leave the study during week 16 (15.8% dropout rate).
The study found that women in the Vibrance Pelvic Trainer group had significant improvement in stress UI scores and significantly better pelvic floor muscle strength. Results also showed the significant difference in improvement in stress UI symptoms occurred earlier (within the first 4 weeks) while using the Vibrance Pelvic Trainer as compared to performing pelvic floor muscle exercises without the device. Researchers posited that accurate recognition of correct muscle contractions may have led to these early results with the prescribed regimen. Better compliance for the Vibrance Pelvic Trainer group may also be contributed to experiencing improvements early in the study. Furthermore, earlier results could have enhanced patient motivation and encouraged continuance, consistency, and overall compliance with the prescribed exercise regimen. These areas were identified as potential areas for further investigation.
Women in the Vibrance Pelvic Trainer group also reported significant improvements in sexual health, specifically orgasm intensity and quality of intimate experience. Additionally, they commented on the Vibrance Pelvic Trainer’s ease of use, comfort, packaging, and clarity of instructions.
Summary
A woman’s knowledge and willingness to pursue consistent pelvic floor muscle home-training remain as obstacles for successful first-line treatment in managing urinary incontinence and related bladder symptoms. With one in four adult women suffering from urinary incontinence, a pelvic floor muscle trainer that assists, educates, and progressively adapts, could make an impactful difference, and improve the quality of life for women.
The Vibrance Pelvic Trainer offers health care providers a clinically proven, practical solution for women seeking a safe, convenient, and easy-to-use at-home treatment for urinary incontinence. The device’s vibrational biofeedback feature informs and trains women to isolate and exercise the right muscle correctly; the three Training Sleeves offer women progressive resistance for gaining muscle strength and endurance; and auditory cues guide women in performing rapid voluntary pelvic floor muscle contractions of variable intensity. Today, only expert clinicians can offer this level of pelvic floor muscle resistance training with accurate biofeedback in formal, in-office, intensive sessions.
Early Vibrance Pelvic Trainer study results support expert clinical experience that forming good pelvic muscle exercise habits help motivate a woman’s overall compliance resulting in improvements in stress UI symptoms, pelvic floor muscle strength, vaginal and bladder support, sexual health, and sensitivity. The Vibrance Pelvic Trainer offers health care providers a viable and validated tool for gaining patient compliance and success with a home-based, self-directed, pelvic floor muscle training program.
For more information, see vibrancepelvictrainer.com
©2018 Vibrance™. All rights reserved. Contents of this publication may not be reproduced without the written permission of Vibrance.
The information contained herein is subject to change without notice.
Appendix
Safety
The Vibrance Pelvic Trainer is FDA-cleared, has gained approval in nine countries, Health Canada and Europe CE mark, and has received the 2012 Medical Design Excellence Award (over-the-counter and self-care category).
| Design | Simple T-shaped design contains a main biofeedback unit and three training sleeves. Biofeedback unit includes two enclosed electrodes – an active vibration biofeedback for the identification of the correct muscles and one for audible exercise guidance. For in-home use. Received the Medical Design and Excellence Award for design and effectiveness in 2012 (Silver Winner) for design and engineering in the Over-the-Counter and Self-Care Category.[24] Set up requires battery charging. Includes no external device interface (e.g., smartphone apps, wireless pairing). |
| Cleaning | Mild soap and rinsing. No peroxide, alcohol, or boiling. Waterproof when the bottom cap is screwed tight. |
| Biocompatibility | Body-safe, sleeves are made of medical-grade silicone rubber tested and deemed safe. Hygienic, phalate-free, and hypoallergenic. |
| Regulatory Review |
FDA clearance, United States[25], European Union, Australia TGA, Canada CMDCAS, UK MHRA Other regulatory clearances include: Singapore HSA, Taiwan FDA, Health Canada, Australia TGA, Kuwait FDA, Europe CE mark, Korea FDA, Saudi Arabia FDA. Can be purchased without a prescription from a medical professional. |
| Performance Testing | ISO 10993 Biocompatibility Tested; ISO 13485 Quality Management System for Medical Devices; IEC 60601 Safety & Effectiveness of Medical Equipment Tested; and IEC 62133 Global Battery Safety. |
Definition of Terms (Adapted from Newman & Wein, 2009)
Apps – An application, especially as downloaded by a user to a mobile device.
Contractibility – The rate of the original rise of the muscle contraction.
Endurance – The time that a sub-maximum muscle contraction can be maintained or repeated before a 50% or more reduction in the power is detected (the muscle contraction is timed until the muscle fatigues.)
Power – The ability of the muscle to “contract-relax” as quickly and strongly as possible, until the muscle fatigues; these are often called “quick flicks.”
Repetitions – The number of repetitions (up to 10) of the muscle contraction of equal force that can be achieved which indicate muscle coordination and function.
Rest – The ability of the muscle to return to a resting state between each contraction.
Strength – Recorded as the peak maximum pressure (the maximal contraction) and the ability to sustain or hold the contraction.
References
[1] Buckley BS, Lapitan MCM. Prevalence of urinary incontinence in men, women, and children-current evidence: findings of the Fourth International Consultation on Incontinence. Urology. 2010; 76(2):265–270.
[2] National Association for Continence. Facts and Statistics. www.forum.nafc.org. Accessed 2017.
[3] Dumoulin C, Hay-Smith EJC, Mac Habée-Séguin G. Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. Cochrane Database of Systematic Reviews. 2014; 5. Art. No.: CD005654. DOI: 10.1002/14651858.CD005654.pub3.
[4] Siegel A. The Kegel Renaissance. J Urol Res. 2016; 3(4):1061.
[5] Milsom I, Altman D, Cartwright R, Lapitan MC, Nelson R, Sillén U, et al. Epidemiology of urinary incontinence (UI) and other lower urinary tract symptoms (LUTS), pelvic organ pro-lapse (POP) and anal incontinence (AI). Incontinence: 5th International Consultation on Incontinence. 2013; 27-43.
[6] Aoki Y, Brown HW, Brubaker L, Cornu JN, Daly JO, Cartwright R. Urinary incontinence in women. Nature Reviews. Disease Primers. 2017; 3,17042. http://doi.org/10.1038/nrdp.2017.42.
[7] Lukacz ES. Patient education: Urinary incontinence treatments for women (Beyond the Basics). Up-to-Date. Jan. 03, 2018.
[8] Bo K, Frawley HC, Hayden BT, Abramov Y, Almeida FG, Berghmans B, Bortolini M. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for the conservative and nonpharmacological management of female pelvic floor dysfunction. Int Urogynecol J. 2017; 28:191-213.
[9] Corcos J. et al. CUA Guideline on Adult Overactive bladder. Can Urol Assoc. 2017; 11(5)142-173.
[10] Reid, Abramson, Blake et al. Urogenital Health Chapter 5. J Obstet Gynaecol Can 2014, Vol 36(9), S38.
[11] American College of Obstetricians and Gynecologists. Physical Activity and Exercise During Pregnancy and the Post-Partum Period. ACOG Committee Opinion: Number 650, December 2015. www.acog.org.
[12] Quaseem A, Dallas P, Forciea MA, Starkey M, Denberg TD, Shekelle P. Clinical Guidelines Committee of the American College of Physicians, Nonsurgical management of urinary incontinence in women: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2014; 161(6): 429-40.
[13] Abrams P, Cardozo L, Wagg A, Wein A (Eds.): Incontinence: Proceedings from the 5th International Consultation on Incontinence. ICUD ICS Publications. 2017; 1445-1628.
[14] Price N, Dawood R, Jackson S. Pelvic floor exercise for urinary incontinence: A systematic literature review. Maturitas. 2010 doi: 10.106/j maturitas.201008.004.
[15] Dumoulin C, Glazener C, Jenkinson D. Determining the optimal pelvic floor muscle training regimen for women with stress urinary incontinence. Neurourology Urodynamics. June 2011; 30 (5): 746-753.
[16] Delgado D, White P, Trochez R, Drake MJ. A pilot randomized controlled trial of the pelvic toner device in female stress urinary incontinence. Int Urogynecol J. 2013; 24(10):1739. doi:10. 1007/s00192-013-2107.
[17] Jean Hailes for Women’s Health. Women’s health information needs in Australia survey. 2015;19.
[18] Kegel AH. Progressive resistance exercise in the functional restoration of the perineal muscles. Am J Obstet Gynecol.1948; 56:238-49.
[19] Newman DK. Pelvic floor muscle rehabilitation using biofeedback. Urologic Nursing. 2014; 34(4): 193-202.
[20] Newman DK, Sung VW, Borello-France D. Structured behavioral treatment research protocol for women with mixed urinary incontinence and overactive bladder symptoms. Neurology Urodynamics, 2018; 37(1);14-20. doi: 10.1002/nau.23244.
[21] Newman DK, Wein AJ. Office-based behavioral therapy for management of incontinence and other pelvic disorders. Urologic Clinics of North America. Nov 2013;40(4):613-35.
[22] Keshtidar M, Behzadnia B. Prediction of intention to continue sport in athlete students: A self-determination theory approach. PLoS ONE. 2017;12(2), e0171673. http://doi.org/10.1371/journal.pone.0171673.
[23] Ong et al. Using the Vibrance Kegel Device with Pelvic Floor Muscle Exercise for Stress Urinary Incontinence: A Randomized Controlled Pilot Study, UROLOGY 86 (3).2015, 487-491.
[24] Vibrance™ Pelvic Trainer Wins Silver in the 2012 Medical Design Excellence Award, 2012. www.vibrance pelvictrainer.com Accessed October 25, 2017.
[25] VibranceTM Pelvic Trainer Receives FDA Clearance, 2014. www.vibrancepelvictrainer.com. Accessed October 20, 2017.